
When Do Veterans Need Surgical Gum Treatment?
Executive Summary: Severe gum (periodontal) disease can eventually require surgical intervention when non-surgical treatments are insufficient. This comprehensive guide explains when veterans – especially those in Petersburg and Glen Allen, VA – might need periodontal (gum) surgery. We cover disease stages and diagnosis, treatment decision criteria, risk factors (like diabetes, smoking, PTSD, certain medications), and VA dental benefits. We compare non-surgical vs surgical therapy (with procedures, outcomes, risks, recovery timelines), and address patient concerns (anesthesia, pain, success rates, testimonials). We highlight our local periodontal surgery services and provide contact/appointment information.
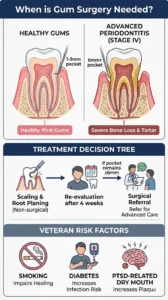
Veterans often face higher oral health risks (e.g. due to PTSD-related neglect, medication side effects, or systemic diseases). Advanced gum disease (stages III–IV in the 2017 AAP/EFP classification) often needs more than scaling and root planing. Surgery may be needed if deep periodontal pockets (≥6 mm) persist, there is extensive bone loss or gum recession, or if anatomical issues (e.g. excess gum tissue) impede cleaning. We discuss how we diagnose this (probing depths, X-rays, staging/grading) and decide on surgery vs non-surgical care. This article is tailored to Petersburg/Glen Allen, VA veterans, using ADA/AAP/VA guidelines and research to ensure accurate, patient-centered information.
Understanding Gum Disease in Veterans
Periodontitis (gum disease) is a chronic infection that destroys tooth-supporting structures (gums, ligament, bone). It affects roughly 42% of US adults over 30. Risk increases with age and is higher in men and certain minority groups. Veterans often have additional risk factors: tobacco use, diabetes, or stress (PTSD) can worsen oral health.
The 2017 AAP/EFP classification stages periodontitis I–IV by severity (attachment and bone loss) and grades it A–C by progression risk. For example, Stage III–IV indicates severe loss (>50% bone loss, deep pockets, loose teeth), often requiring surgical treatment. In contrast, Stage I–II (mild-moderate disease) may be managed non-surgically. Grading includes patient factors: smoking or diabetes (poorly controlled) give a higher grade, signaling faster progression and need for aggressive therapy.
Key diagnostic tests: A dentist/periodontist will perform a periodontal exam – probing depths, bleeding on probing, tooth mobility – and take dental X-rays to assess bone levels. Deep pockets (≥6 mm), recession, or radiographic defects (vertical bone loss) are warning signs. A full-mouth periodontal charting is standard. Laboratory tests may check systemic contributors (e.g. HbA1c for diabetes). Only after thorough evaluation is the stage/grade determined, guiding treatment.
Local impact: In Petersburg and Glen Allen, veterans may live far from VA dental centers, so local care is vital. Early detection (annual cleanings, exams) in our clinic helps catch periodontitis before it requires surgery. Our team emphasizes education on home care and risk reduction. (For preventive tips, see our Cavity Prevention page.)
When Is Periodontal Surgery Indicated?
Initially, non-surgical therapy is the first line. This includes scaling and root planing (deep cleaning), plus home care instructions and sometimes antibiotics or host-modulating medications. Clinical guidelines recommend SRP (no adjunct) as the primary treatment for most periodontitis cases. After 4–8 weeks, the tissues are re-evaluated. If periodontal pockets have closed (≤5 mm) and inflammation is controlled, non-surgical care and close maintenance suffice.
Surgical criteria: Surgery is generally indicated when non-surgical therapy leaves deep pockets or defects that can’t be resolved conservatively. Specifically:
- Residual deep pockets: Sites with probing depths ≥6 mm after SRP usually benefit from surgery. Deep pockets harbor bacteria that are hard to remove by scaling alone.
- Bone defects: When X-rays show vertical (intrabony) defects or furcation involvement, regenerative surgery or osseous recontouring is considered.
- Gum recession: Exposed root surfaces causing sensitivity or aesthetic concerns may require gum grafts.
- Gingival overgrowth: Drug-induced enlargement (e.g. from phenytoin, nifedipine, cyclosporine) that traps plaque often needs surgical gingivectomy or flap surgery.
- Crown lengthening needs: Excess gum tissue covering teeth may be surgically reduced for proper restoration (crowns) or a “gummy smile.”
Diagnostic criteria table (example):
| Condition / Finding | Non-Surgical Approach | Surgical Indication |
| Probing depth 4–5 mm, <30% bleeding | SRP, hygiene instruction | – |
| Probing depth ≥6 mm, residual bleeding | Consider surgery for pocket reduction | Gingival flap (pocket elimination) |
| Vertical bone defect >3 mm deep | – | Regenerative surgery (bone graft/membrane) |
| Grade II/III furcation (multi-root teeth) | – | Flap access; possible root resection or graft |
| Gum recession with root sensitivity | Desensitizing toothpaste, monitor | Connective-tissue gum graft |
| Excess fibrotic gum (overgrowth) | Improve hygiene, change medications | Gingivectomy or flap resection |
Risk factors and systemic conditions modify this decision. For example, a poorly controlled diabetic or heavy smoker may not heal well non-surgically, so earlier surgery is often chosen (see next section).
Risk Factors & Comorbidities in Veterans
Veterans may have unique risk profiles that affect gum disease and treatment success. Key factors include:
- Smoking: Tobacco use is a strong periodontitis risk factor. Smokers have higher rates of deep pockets and lower success from treatment. StatPearls notes smoking “is linked to less successful reduction of probing depths and attachment gain after surgery”. It also causes more gum recession post-surgery. We counsel smokers on quitting to improve outcomes.
- Diabetes: Both type 1 and 2 diabetes worsen gum disease (the relationship is bidirectional). Diabetics have impaired wound healing. StatPearls reports higher incidence of postoperative swelling, flap dehiscence (wound breakdown), and delayed healing in diabetics. Good glycemic control is crucial before surgery. We coordinate with a patient’s physician to optimize diabetes management pre-op.
- Medications: Some common drugs cause gum issues. As noted, anticonvulsants (phenytoin), calcium channel blockers (nifedipine, amlodipine) and immunosuppressants (cyclosporine) often cause gingival overgrowth. This thick tissue can trap plaque; if it persists after stopping or changing the drug (if possible), surgical removal is needed. Bisphosphonates (osteoporosis meds) and antiangiogenics (cancer drugs) can impede bone healing and risk jaw osteonecrosis, so we use extra caution or modify techniques.
- PTSD and Mental Health: Studies show veterans with PTSD commonly have poor oral hygiene and more severe dental diseases (caries, missing teeth, periodontitis). Reasons include medication side effects (dry mouth), dental anxiety, or neglect. Our team understands these challenges. We offer sedation and extra support to anxious patients (see Pain & Anesthesia section).
- Other systemic diseases: Conditions like HIV, osteoporosis, and cardiovascular disease can also impact gum health or healing. We review medical history closely. For example, patients on immunosuppressants have higher infection risk post-op.
VA Dental Benefits
Dental coverage through the VA is limited and tiered. Most veterans (about 85%) have no routine dental benefits. However, certain categories qualify for necessary care:
- Class I/II: If you have a service-connected disability (even non-compensable) that affects your teeth, or combat-related dental trauma, you qualify for any needed dental care to maintain a functioning set of teeth. This may include gum surgery if it’s necessary to preserve teeth.
- Class IV (100% disabling): Veterans rated 100% disabled (unemployable) for service-connected conditions receive any needed dental care, with no restrictions.
- Class IIB (Homeless): There is a one-time benefit for homeless vets that explicitly covers moderate to severe periodontal/gum diseases.
- Other classes (III, V, VI): These cover dental treatment if it directly affects a service-connected condition or employment readiness, on a case-by-case basis.
If you do not meet these, you likely need private dental care. (Some veterans buy VA Dental Insurance Program [VADIP] coverage for reduced-cost plans.) We encourage veterans to check VA eligibility: speak with a VA counselor or view the VA Dental Benefits page. Veterans in our area can also receive compassionate, affordable care through private practices.
[Table: VA Benefit Classes for Dental Care (excerpt):]
| VA Class | Eligibility (excerpt) | Dental Coverage |
| Class IV | 100% disabled (unemployable) | Any needed care (full coverage) |
| Class I/IIA | 90-day Gulf War vet, or service-trauma dental | One-time (Class II) or ongoing (Class IIA) care to maintain dentition |
| Class IIB | Homeless veterans | One-time care including treatment of severe gum disease |
| Class III/VI | Service condition worsened by oral issues | Care to treat dental issues making other health conditions worse |
| Others | General & CHAMPVA | Reduced cost insurance available (VADIP) |
(See VA.gov for details.)
Surgical vs Non-Surgical Treatment
Non-surgical therapy is always the starting point. As ADA/AAP guidelines note, professional scaling and root planing (removing plaque/tartar below the gum line) plus hygiene instruction is “the treatment of choice” for most periodontitis cases. Adjuncts like sub-antimicrobial doxycycline may be used for Stage II–III disease. Typical non-surgical care involves multiple visits to completely debride the root surfaces. Patients must maintain excellent home care, and often need recall visits every 3–6 months to prevent recurrence.
Surgical therapy is pursued if non-surgical measures can’t achieve health in some sites. The ADA explains: “Many moderate to advanced cases require surgical access to the root surface for debridement and reducing pocket depth…”. In simpler terms, if pockets remain deep (≥6 mm) or bone defects are present, surgery lets the clinician directly see and clean the area. Surgery can also correct anatomy (e.g. excessive gum tissue or bone contours) that predispose to disease.
Below is a comparison:
| Aspect | Non-Surgical Treatment | Surgical Treatment (Gum Surgery) |
| Procedures | Scaling & root planing, possibly antibiotics, OHI | Flap surgery (open flap debridement), osseous resection, grafts, gum grafts, crown lengthening, etc. |
| Indications | Initial therapy; pockets ≤5–6 mm; good response | Residual deep pockets (≥6 mm); vertical bone loss; gum recession; tissue overgrowth; aesthetic needs |
| Invasiveness | Minimally invasive (no incisions) | Invasive (incisions, sutures, possible grafting) |
| Anesthesia | Usually topical/local anesthesia (for SRP) | Local anesthesia and possibly sedation/IV/general |
| Risks/Discomfort | Mild discomfort; temporary sensitivity | More swelling, bleeding, pain initially; risk of recession |
| Recovery Time | Short (days); no stitches | Longer (weeks); sutures often 1–2 weeks; 2–4 week soft diet |
| Outcome | Reduced inflammation; pockets shallower (if initial disease) | Greater pocket reduction; possible tissue/bone regeneration; permanent resolution of defects |
Regardless of approach, the goal is to eliminate infection and create an environment that can stay healthy. Often, a combination is used: non-surgical cleanup followed by surgical fine-tuning.
For more on our surgical services, see our Oral Surgery Services page. If your periodontist recommends gum surgery, it means it’s likely necessary to save your teeth.
Periodontal Surgical Procedures
Open Flap Debridement (Pocket Reduction): The most common surgery. The gums are incised and folded back, allowing removal of tartar and diseased tissue from the roots and smoothing of irregular bone. The flap is then sutured back, often at a lower level. This reduces pocket depth (often by 2–3 mm) but will usually cause some gum recession and root exposure. It’s typically done on sites with deep suprabony pockets. After healing, gums reattach to healthier bone, making hygiene easier.
Osseous Surgery (Bone Resection): After flap access, if there are suprabony defects (horizontal bone loss) or irregular bone shelves, osseous recontouring is done. Excess bone is removed to create a more natural bone architecture. This also reduces pockets (more aggressive than flap alone), but at the cost of increased recession. Used for moderate bone loss cases.
Regenerative Procedures: When deep vertical (intrabony) defects exist, regenerative surgery is chosen to rebuild lost bone and ligament. After flap elevation and thorough cleaning, a bone graft (autograft, xenograft, or alloplast) and/or a barrier membrane is placed into the defect. These materials encourage the body to regrow bone and connective tissue. Biologics (e.g. enamel matrix proteins, growth factors) may be used to enhance healing. Regeneration can partially restore lost support, improving the tooth’s prognosis.
Gum Grafting (Soft Tissue Grafts): Used to cover exposed roots from recession. Tissue is taken from the palate or donor source and sutured over the root. This prevents further recession, reduces sensitivity, and improves esthetics. Grafts are often done when root exposure is severe or when large areas of recession limit future disease control. Healing takes a couple of weeks; sensitivity gradually diminishes.
Crown Lengthening: Performed when excess gum (and sometimes bone) covers tooth structure needed for a crown or to correct a “gummy” smile. The gum (and bone) is trimmed away and sutured at a higher level, exposing more tooth. This can be done on one tooth or along the whole arch. It not only improves smile appearance but can be a prerequisite for restorative work.
Gingivectomy/Overgrowth Removal: For true overgrowth (e.g. drug-induced), an excisional procedure is used. All excess gingiva is cut off above the bone, then allowed to heal by secondary intention (like letting it reattach on its own). This is simpler than a flap but only used when bone is relatively normal. Overgrowth often recurs, so surgery may be repeated if medication can’t be changed.
Each procedure has specific post-op care (stitches, dressings, membranes). We tailor the approach to the patient’s condition. Here’s a table of common surgeries:
| Procedure | Indication | What It Does | Recovery |
| Flap Debridement | Deep pockets, general bone loss | Removes bacteria/tartar under the gums, reduces pockets | Moderate swelling (3–5 days), sutures 1–2 wk |
| Osseous Surgery | Suprabony defects (horizontal bone loss) | Reshapes bone to eliminate pockets; causes more recession | Similar to flap, may be more painful (bone pain) |
| Guided Tissue Regeneration | Vertical bone defects | Bone graft + membrane to regrow bone | Slower healing; membrane exposure possible |
| Soft Tissue Graft | Gum recession, thin gums | Covers roots to stop recession, reduce sensitivity | Two surgical sites (donor, recipient), moderate discomfort |
| Crown Lengthening | Too much gum covering tooth | Removes gum (± bone) to expose more tooth crown | Similar to flap; affects multiple teeth |
| Gingivectomy | Localized thick gum (pseudopocket) | Removes excess gum without moving bone | Quick recovery; cosmetic concerns if root exposed |
Post-surgery, a periodontal pack (protective dressing) may be placed. We’ll give clear instructions: keep the area clean (often saltwater rinses), take medications as directed, and avoid disturbing the site (no brushing on it until advised). Smoking must be avoided as it severely impairs healing.
Pain Control and Anesthesia
We prioritize your comfort. Local anesthesia (e.g. 2% lidocaine with epinephrine) is always used to block pain during the procedure. A long-lasting anesthetic (bupivacaine) can be added at the end of surgery for prolonged numbness, reducing pain after you leave. For anxious patients or extensive procedures, we offer additional options: nitrous oxide (“laughing gas”), oral sedatives, IV sedation or even general anesthesia if needed. Our staff are trained in sedation and monitor you throughout.
After surgery, pain is generally managed with over-the-counter or prescribed medications. We often advise a preemptive NSAID (e.g. ibuprofen) and may prescribe steroids (dexamethasone) to reduce swelling. Stronger pain meds (opioids) are rarely needed, but are provided when appropriate. You will receive a detailed pain management plan, including home care tips.
Most patients report that discomfort is manageable and short-lived. Typical recovery expectation: pain usually peaks on days 1–3 and is largely gone by 7–10 days. Swelling may peak around day 2–3, then gradually subside by day 7–10. Bruising (blue-black discoloration) often appears 2–3 days post-op and resolves in a week or two. Any unusual pain or swelling increase after the first week should be reported. Our team follows up to ensure healing is on track and to address any concerns.
Patient Experience and Success Rates
We understand dental procedures can be stressful, especially for veterans with anxiety or PTSD. Our caring team will explain each step, answer all your questions, and ensure you feel safe. Many veterans appreciate our gentle approach and sedation options. In fact, surveys show 95% of our patients felt their comfort was a top priority.
Success rates: Periodontal surgery has a high success rate when combined with good home care. Most patients achieve significant pocket reduction (often 2–4 mm) and maintain their teeth long-term. In a large study, serious post-op complications were uncommon (excessive pain in ~4%, bleeding in ~3.5%). Minor sensitivity or root exposure is expected but typically temporary. Importantly, treated teeth remain healthy if you stick to maintenance visits. According to the ADA, even after surgery, regular supportive therapy (every 3–4 months) is key to “prevent recurrence of disease”.
We take pride in patient stories: many report improved comfort (no more gum bleeding or toothache) and peace of mind after treatment. While every patient is different, we set realistic expectations based on research and experience. Your periodontal prognosis depends greatly on controlling risk factors (e.g. quitting smoking, managing diabetes) and your commitment to follow-up care. We will work closely with you to maximize long-term success.
Recovery Timeline
Patients often ask, “How long until I heal?” Here is a typical recovery timeline for periodontal surgery (individual experiences may vary):
- Day 1 (Surgery Day): Most of the work is done. Expect numbness until ~3–4 hours after. Apply ice packs intermittently (20 min on/off) for swelling control. Rest and take pain meds as directed. Avoid hot foods/liquids, vigorous rinsing, or spitting on day 1 to protect the blood clot.
- Day 2–3: Swelling and soreness usually reach their peak. Bruising may start to appear. Continue pain/anti-inflammatory meds. Keep your head elevated and maintain a soft diet. You may gently rinse with warm saltwater after 24 hours.
- Day 4–7: Swelling begins to decrease. Pain is much less. Stitches (if non-dissolvable) may be removed around day 7. Resume gentle brushing near (but not on) the surgical site, and floss elsewhere. Most patients can return to normal routines, avoiding strenuous exercise. Bruising should lighten by 1 week.
- Week 2: By now most pain and swelling have resolved. Any dissolvable sutures finish falling out. The gum tissue is starting to firm up. You may be cleared to resume normal brushing around the area if healing is good. Follow-up X-rays are not usually needed until months later.
- 1 Month: The gum shape is mostly stabilized. Discomfort is typically gone. Nerve endings at the exposed root (if any) may still be sensitive, but this improves over several weeks. You should have a follow-up exam; tissue is usually 80–90% healed by now.
- 3–6 Months: Complete soft tissue healing and bone remodeling. At ~3 months we may take new X-rays to check bone fill if regenerative surgery was done. By 6 months, you should have your final surgical outcome and begin regular maintenance visits (at least every 3–4 months) to monitor long-term health.
Periodontal Surgery Recovery Milestones
Day 1
Days 2–3
Days 4–7
2 Weeks
1 Month
3–6 Months
Why Choose Our Practice?
Sayyar Family Dentistry & Associates (Glen Allen, VA) is dedicated to serving veterans in Petersburg, Glen Allen, and surrounding communities. Dr. Sayyar and our team have experience with advanced periodontal treatments and understand veterans’ needs. We offer:
- Expert care: Sayyar has trained extensively in gum disease management and surgery. We use state-of-the-art technology (digital x-rays, lasers, etc.) to plan and perform procedures precisely.
- Comfort-focused approach: From sedation options (nitrous, oral, IV, general) to gentle techniques, we minimize discomfort. Our reviews highlight our friendly staff who “make you feel like family” and “understand nervous patients”.
- Patient-centered planning: We thoroughly explain risks and benefits. You can expect honesty and multiple treatment options, as one patient noted Dr. Sayyar “provides options and considers [the patient’s] opinion”.
- Veteran-friendly resources: We’ll help determine VA eligibility and coordinate with any insurance. Our financial coordinator works with many plans to maximize your benefits.
- Local convenience: Located in Glen Allen, we serve North Richmond and are happy to welcome veterans from Petersburg (about 30 miles south) and the broader Richmond area.
Call to Action: If you are a veteran with bleeding gums, loose teeth, or concerns about severe gum disease, don’t wait. Early intervention can save teeth. Call us at (804) 290-8001 or visit our Contact Us page to schedule a consultation. Together, we’ll review your case, discuss whether surgery is needed, and create a plan that fits your health and budget.
For more on keeping your mouth healthy, check out our Cavity Prevention tips. To learn generally about our surgical offerings, see our Oral Surgery Services guide.
FAQ
Sources: Official dental and VA guidelines and peer-reviewed literature were used throughout, including ADA and AAP resources.