
Diabetes & Gum Disease: Petersburg & Glen Allen Veterans’ Oral Health
Executive Summary: Veterans with diabetes face notably higher risk for periodontal (gum) disease due to intertwined metabolic and immunologic factors. Elevated blood sugar in diabetes alters saliva and blood vessels, impairs white blood cells, and fuels chronic inflammation, all of which worsen gum infection. Conversely, active gum disease creates systemic inflammation that raises blood sugar, creating a harmful two-way cycle. Because Virginia’s veterans are older and have more diabetes than the general public (22% vs 12% nationally), their periodontal burden is significant: one survey found 42% of vets reported gum treatment or bone loss vs 27% of nonveterans. This article reviews how diabetes drives gum disease (and vice versa) via microvascular changes, immune dysfunction, oral microbiome shifts and inflammation. It covers epidemiology (including veterans’ data), typical clinical findings, and the diabetes-oral health link. We summarize screening and care recommendations (medical-dental coordination, glycemic control, periodontal therapy, prevention), and highlight local resources in Petersburg and Glen Allen (VA dental clinics, community dental centers). Patient advice focuses on self-care and warning signs. We discuss how gum disease impacts systemic health. Tables compare key periodontal risk factors and integrated care strategies, and a mermaid flowchart outlines a coordinated timeline of diabetes–dental care. Internal links to Dr. Sayyar’s practice pages are provided for local readers. Veteran-friendly call to action: veterans are encouraged to schedule regular dental exams and blood sugar checks in tandem, and to call Sayyar Family Dentistry for coordinated care.
Pathophysiology: How Diabetes Drives Gum Disease
Diabetes fundamentally alters tissue metabolism and the immune response, creating a fertile ground for periodontal infection. Chronically high glucose leads to non-enzymatic glycation of proteins, forming advanced glycation end-products (AGEs) that accumulate in blood vessel walls. In the gums, AGE-modified collagen thickens capillary basement membranes, impairing oxygen and nutrient flow to the periodontal tissues. This microvascular damage weakens the gum’s resistance to bacteria. At the same time, hyperglycemia dysregulates immune cells. Studies show diabetic patients have impaired neutrophil (polymorphonuclear leukocyte, PMNL) chemotaxis, adherence and phagocytosis. In other words, their white blood cells are sluggish in reaching and engulfing periodontal pathogens. These factors cause diabetic gum tissue to be more susceptible to chronic infection and poor healing.
High blood sugar also alters saliva and plaque: diabetics often have xerostomia (dry mouth) and glucose-rich saliva, which promote bacterial overgrowth. Some studies find diabetic patients have higher counts of the “red complex” periodontopathogens (e.g. P. gingivalis, T. denticola, T. forsythia) in subgingival biofilms, possibly because extra nutrients and reduced saliva clearance favor these germs. Regardless of precise bacterial shifts, the result is more aggressive periodontal breakdown.
Perhaps most importantly, diabetes provokes a hyper-inflammatory state. Elevated glucose and AGE–RAGE signaling activate NF-κB and other pathways in gum tissues, boosting local cytokines (IL-1β, IL-6, TNF-α). Inflammatory enzymes (MMPs, collagenases) and oxidative stress surge, accelerating destruction of the periodontal ligament and alveolar bone. Experimental work shows diabetic animal models have exaggerated bone loss when challenged with periodontitis pathogens. Clinically, poor glycemic control correlates with higher gingival crevicular fluid levels of IL-1β and TNF-α, and greater tissue damage. In summary, diabetes fuels both the quantity and virulence of inflammation in gum tissue.
Importantly, the link is bidirectional. Inflammation from periodontal infection spills into the bloodstream, elevating systemic C-reactive protein and cytokines that worsen insulin resistance. In practice, active gum disease often raises blood sugar levels, making diabetes harder to manage. The American Diabetes Association notes that uncontrolled gums can contribute to higher HbA1c, and conversely that good diabetes control lowers gum disease risk. A 2018 systematic review confirms periodontitis is associated with elevated HbA1c and more diabetic complications in Type 2 diabetics.
In essence, diabetes creates a vicious cycle: microvascular injury + immune dysfunction + inflammation in the gums allow bacteria to flourish, while gum infections magnify inflammation that impairs metabolic control. Together these pathophysiologic changes explain why people with diabetes – including veterans – are far more prone to severe, rapidly progressing periodontitis (gum disease) than those without diabetes.
Epidemiology & Veteran-Specific Data
Periodontitis is extremely common overall, but even more so among people with diabetes and veterans. National data show roughly 46–50% of U.S. adults 30+ have some degree of periodontal disease, rising to about 70% of seniors 65+. Veterans tend to be older than the general population, and male veterans have higher rates than civilian peers. The VA notes that U.S. veterans are more likely to carry risk factors: e.g. smoking (which raises PD risk to ~64% in smokers vs ~43% in nonsmokers).
Crucially, veterans also have higher diabetes rates. A CareQuest analysis found 22% of veterans in a NHANES sample reported having diabetes, versus 12% of non-veterans. By contrast, civilian diabetes prevalence is ~11.3% (CDC 2023). More diabetes means more gum disease. In fact, the same veteran survey reported 41.7% of veterans had bone loss or past gum treatment, compared to 27% of non-veterans. (A small difference remained after adjustment for age, suggesting veterans carry a higher periodontal burden.)
Regionally, Virginia’s veterans echo national trends. Although state-specific periodontitis rates are scarce, many risk factors cluster in Petersburg/Glen Allen: older age cohorts, histories of smoking, and a substantial retiree population from the military. National VA studies (and CDC data) consistently show that diabetic individuals are two to three times more likely to develop severe periodontitis than nondiabetics. For example, the ADA emphasizes that diabetics have 2–3× higher odds of gum disease compared to healthy controls. The implication: Petersburg and Glen Allen veterans with diabetes constitute a particularly high-risk group.
Key Takeaways on Epidemiology: Nearly half of adults overall have gum disease, but rates are even higher in seniors and in those with diabetes. Veterans – who smoke more and have more diabetes – report more periodontal problems (42% vs 27% in civilians). Studies confirm diabetes roughly doubles or triples the risk of moderate-to-severe periodontitis, especially when blood sugar is poorly controlled.
Clinical Presentation and Complications in Diabetics
Gum disease in a diabetic patient often looks like “textbook” periodontitis but with greater severity and faster progression. Clinically, one sees typical signs: red, swollen and bleeding gums; bad breath (halitosis); gum recession; and deep periodontal pockets. However, in diabetics these can appear earlier and worsen rapidly. For instance, diabetics frequently present with diffuse gingival inflammation that does not subside after basic cleaning. Loose or drifting teeth are more common complications; uncontrolled diabetes can cause even minor gingivitis to escalate into generalized periodontitis with significant bone loss within a short time.
Diabetic periodontal lesions also tend to be more fibrotic and fibrotic, reflecting chronic inflammation and altered collagen metabolism. You may see more gingival abscesses or necrotizing lesions in poorly controlled diabetics. Wound healing in the mouth is sluggish: extractions, surgeries or even deep cleanings often heal more slowly and unpredictably. This poor healing is driven by impaired growth-factor signaling and reduced blood flow (from earlier AGE effects).
The systemic consequences of diabetic gum disease are troubling. Studies show that severe periodontitis in diabetes is linked to worse retinopathy, nephropathy, and even cardiovascular outcomes. For example, one meta-analysis found that diabetic patients with periodontitis had higher odds of diabetic complications and nearly double the gingival fluid IL-1β levels compared to diabetics with healthy gums. Moreover, any active infection, including periodontal abscess, can trigger a spike in blood sugar. Chronic periodontal inflammation exacerbates insulin resistance, contributing to the “failure” of diabetic control. Veterans with long-standing diabetes and gum disease often experience cycles of hyperglycemia and infection: each aggravates the other.
Examples of Complications: Diabetics with periodontal disease lose more teeth on average, and often have a pattern of bone loss around teeth that correlates with their HbA1c level. They also face a higher risk of periodontal abscesses (deep pus pockets) and a rarer condition called necrotizing periodontitis if immune defense is severely impaired. In turn, poorly managed gum disease can lead to complications elsewhere: elevated systemic inflammation from the gums has been implicated in worsening heart disease, stroke risk, poor wound healing (diabetic ulcers), and even pneumonia risk in diabetics.
Screening and Management Recommendations
Effective care of diabetic veterans requires close coordination between medical and dental teams. Medical providers should screen diabetic patients for oral symptoms routinely, and vice versa dentists should ask diabetic patients about blood sugar control. Current ADA guidelines (2025 Standards of Care) explicitly recommend annual referral for dental examination for all diabetic patients. The VA also advises that any diabetic patient should see a dentist every 3–6 months for periodontal evaluation, rather than the usual once-yearly visit. At minimum, a thorough periodontal exam (probing depths, attachment levels, radiographs) is indicated at each routine dental visit for diabetics.
Key management strategies are summarized below:
- Optimize Glycemic Control: Tighter blood sugar control (HbA1c <7%) reduces the severity of periodontal disease. For example, uncontrolled diabetes often causes dry mouth and high salivary glucose, which feed plaque bacteria. Managing diet, medications and lifestyle to stabilize glucose will directly reduce oral infection risk. Endocrinologists and primary care providers should adjust diabetes therapy if periodontal inflammation is present.
Rigorous Oral Hygiene: Patients must brush twice daily with fluoride toothpaste, floss daily, and possibly use interdental cleaners or antiseptic mouthwashes. Good home care is the first line of defense.
- For veterans managing both diabetes and oral health, reinforcing that “twice-a-day brushing plus daily flossing” can significantly lower plaque levels is essential. Dentists can teach proper technique and consider powered brushes if dexterity is an issue.
- Frequent Professional Cleanings: Standard cleanings (prophylaxis) at 6-month intervals may need to be every 3-4 months for diabetic patients, especially if periodontitis is active. Scaling and root planing (deep cleaning of pockets) is indicated for any periodontitis. Adjuncts like local antibiotics or antimicrobial rinses (e.g. chlorhexidine) may be used to target stubborn bacteria. Clinics might schedule combined visits: see the primary care physician and dentist on the same day to improve follow-through.
- Medical-Dental Coordination: Dental and medical providers should communicate. For example, a dentist finding uncontrolled periodontal disease should notify the patient’s physician or suggest retesting HbA1c. Similarly, if a PCP learns a diabetic patient had a bad dental infection, they may temporarily alter medications or diet. These roles complement each other: the dental team focuses on infection control and oral inflammation, while the medical team targets systemic glucose and risk factors (like hypertension or lipids).
- Lifestyle Interventions: Both providers should counsel on tobacco cessation (smoking synergizes with diabetes to worsen periodontitis) and stress reduction (chronic stress can spike blood sugar and impair immunity). Nutrition advice overlaps: a low-sugar, balanced diet helps control diabetes and reduces oral acidity.
- Preventive Fluoride and Sealants: In addition to gum care, prevention of caries is relevant since diabetics are prone to dry mouth and cavities. Providers may apply fluoride varnish or recommend fluoride rinses, and pediatric patients (or young adults with wisdom teeth) can get sealants.
- Medication Considerations: Some diabetic medications (e.g. bisphosphonates for osteoporosis or steroids) may affect periodontal health. Dentists should take a thorough medical history and coordinate with physicians when planning surgeries or extractions (e.g. checking bleeding risk or adjusting antihypertensives).
The table below compares key periodontal disease risk factors, highlighting diabetes-specific factors:
| Risk Factor | Effect/Notes |
| Hyperglycemia (HbA1c) | Chronic high glucose leads to AGEs in gums (microvascular injury) and fuels inflammation. |
| Immune Dysfunction | Diabetes impairs neutrophil function (chemotaxis, phagocytosis), weakening infection defense. |
| Smoking | Additive risk: many veterans smoke. Tobacco worsens periodontal breakdown (shown risk ~64% vs 43%). |
| Age | Older adults have far higher prevalence of periodontitis (up to 70% in 65+). |
| Poor Oral Hygiene | Plaque biofilm is the initiating factor. If not removed, it causes chronic gingival infection. |
| Socioeconomic Status | Lower income/education correlates with higher PD rates (poverty <\, 65% prevalence). |
| Genetics / Family History | Certain gene variants (e.g. IL-1) increase susceptibility, though less controllable. |
| Medication / Comorbidities | Meds causing dry mouth (antidepressants), or other systemic illnesses (HIV, etc) can exacerbate risk. |
The following table outlines strategies to manage diabetic periodontal risk, delineating dental vs. medical roles:
| Strategy | Dental Care | Medical Care |
| Glycemic Control | Monitor A1C reports, stress glucose spikes during treatment | Adjust medications or insulin; treat diabetes optimally |
| Oral Hygiene Instruction | Demonstrate brushing/flossing, prescribe aids if needed | Reinforce lifestyle/diet to support oral health |
| Periodic Exams/Cleanings | Prophylaxis every 3–4 months; screen for early gingivitis | Refer diabetic patients for extra dental visits |
| Periodontal Therapy | Perform scaling/root planing, flap surgery as needed | Evaluate for systemic antibiotics if severe (consult PCP) |
| Smoking Cessation | Advise quitting, provide support resources | Provide counseling, medications to help quit |
| Interprofessional Communication | Update PCP on oral findings, send treatment summaries | Update dentist on patient’s diabetes status and meds |
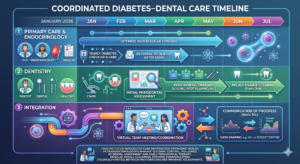
This mermaid chart illustrates a sample timeline for integrating care: PCPs and endocrinologists manage glycemic control and annual diabetes reviews, referring patients promptly to dentistry for evaluation. Dentists perform thorough exams and treatment (scaling, root planing) early in the year, with follow-up cleanings. Periodic communication (telehealth or notes) ensures blood sugar trends and pocket depths inform adjustments by all providers.
Local Resources & Referral Options
Veterans in Petersburg and Glen Allen, VA have several nearby options for dental care, including VA facilities and community clinics:
- Sayyar Family Dentistry (Glen Allen): Dr. Seen Sayyar offers comprehensive dental and periodontal care in Glen Allen. Patients can learn about preventive strategies on our [Cavity Prevention] page and schedule exams via our [Contact page]. The practice’s address (5231 Hickory Park Dr) and phone are listed on our site.
- Southside Dental Cares (Petersburg): A local practice in Petersburg serving veterans. Their team is dedicated to high-quality dental procedures for area residents. Phone (804-732-8557) and service area (Petersburg, Colonial Heights) are on their site.
- United Smiles (Multiple Locations): A regional dental group with an office at 34 Medical Park Blvd, Petersburg (tel. 804-894-9393) and one at 5332 Wyndham Forest Dr, Glen Allen (tel. 804-999-9099). They offer everything from cleanings to periodontal therapy.
- McGuire VA Medical Center (Richmond): Part of the Central Virginia VA Health Care System, the Hunter Holmes McGuire VA has on-site dental services. The McGuire Dental Service (1201 Broad Rock Blvd, Richmond) treats eligible veterans and can manage periodontal issues, often in coordination with the veteran’s PCP. Phone: (804) 675-5000.
- Community Dental Clinics: Nonprofit clinics in the region provide low-cost care. Goochland Cares (2999 River Road West, Goochland) offers dental treatments by appointment. The Lucy Corr Foundation Dental Clinic in Chesterfield provides free dental services one day a week. Both are within ~20 miles of Glen Allen/Petersburg. The Virginia Dental Association Foundation (office in Glen Allen) runs mobile dental units and events for underserved communities.
- Other Options: VA teledentistry and mobile clinics occasionally run clinics. Veterans without VA dental eligibility can often seek care at Federally Qualified Health Centers (e.g. local Health Brigade, GoochlandCares) which may offer sliding-scale fees or referrals for periodontal care.
Veterans should ask their PCP or VA coordinator for guidance on VA dental benefits. Many VA programs cover extractions, periodontal therapy and emergency care for enrolled veterans. Non-VA community providers above can also assist uninsured vets, and Sayyar Family Dentistry offers new-patient appointments (contact info on our [Home] and [Contact] pages) for veterans ready to establish care.
Patient Advice: Protecting Your Gums as a Veteran
Veterans managing diabetes can take many practical steps at home to protect their gums:
- Daily Home Care: Brush at least twice daily with fluoride toothpaste and floss once a day. Aim to remove all plaque each day, especially along the gumline. (The image below illustrates proper flossing technique.) Consistent flossing is critical for diabetics because flossing disrupts plaque biofilm that could otherwise feed infection.
- Monitor for Warning Signs: Regularly check your gums for redness, swelling, bleeding, or any receding gum margins. Loose teeth or gaps between teeth are red flags. Bad breath that persists despite good hygiene can signal an infection. If you notice any of these signs, don’t wait for your next scheduled visit – call your dentist. Early treatment can prevent irreversible damage.
- Control Blood Sugar Religiously: Aim for tight glycemic control as advised by your physician. Log your blood sugars, follow meal plans, and take medications/supplements faithfully. Good diabetes control not only protects your eyes and kidneys but also makes your mouth healthier.
- Quit Smoking: If you smoke or vape, seek help to quit. Smoking greatly worsens gum disease and reduces blood flow to healing gums. VA resources (e.g. “Quit Tobacco” programs) can help veterans kick the habit, which benefits both diabetes and oral health.
- Regular Check-Ups: Keep both medical and dental appointments. Schedule dental cleanings at least every 6 months, or every 3–4 months if your dentist recommends due to active gum issues. Always inform your dentist that you have diabetes and how well it is controlled.
- Maintain Hydration: Drink plenty of water to combat dry mouth. Carry sugar-free gum or saliva substitutes if dry mouth is a problem, to help wash away bacteria.
- Nutrition and Oral Environment: Limit sugary snacks and drinks, which feed bacteria. A balanced diet rich in vegetables and proteins supports healing. Occasionally rinsing with an antimicrobial mouthwash (alcohol-free) can help reduce bacteria count.
- Medication Awareness: Some diabetes medications can influence oral health (e.g., SGLT2 inhibitors may cause dry mouth or increase oral infections). Tell your dentist all your meds and over-the-counter supplements. They may recommend extra measures (fluoride gel, more frequent cleaning) accordingly.
Veterans with mobility or access issues can ask about transportation options; the VA and local Disabled American Veterans chapters often provide shuttle or volunteer driver services for medical and dental appointments. Stay proactive: treating mild gingivitis early can prevent major complications. Diabetic veterans should view the dentist as part of their diabetes care team.
Implications for Overall Health
Gum disease is not just “a mouth problem” – it influences whole-body health, especially in diabetic patients. Chronic periodontal inflammation contributes to the inflammatory burden that drives many diabetes complications. For instance, periodontitis has been linked to higher rates of heart disease and stroke. In one study of veterans, those with both diabetes and periodontitis had more advanced cardiovascular disease markers. Poor oral health also impairs quality of life (difficulty eating, sleep disruption from pain) and can worsen nutritional status.
Conversely, uncontrolled diabetes makes conditions like periodontal abscesses or oral candidiasis (thrush) more likely. Some veterans on immunosuppressive diabetes regimens (like prednisone for an autoimmune complication) are at risk for rare gum diseases.
Importantly, addressing periodontal disease can improve systemic health. Periodontal therapy has been shown to lower HbA1c by about 0.4% on average in the short term. This is a clinically significant drop – comparable to adding a second diabetes medication for some patients. Thus, treating gum disease can help reduce microvascular complications like kidney damage and retinopathy, and may ease the strain on the heart and nerves.
Finally, periodontal infections can act as an infection reservoir that weakens immune defenses. In the context of diabetes, which already impairs healing, this means even minor oral infections can escalate or contribute to illnesses (like pneumonia in bedridden patients). For aging veterans, who may have other comorbidities (COPD, renal insufficiency), controlling gum disease is a vital piece of a holistic health strategy.
Call to Action
Veterans in the Petersburg–Glen Allen area should take prompt action on gum health. Early periodontal disease is treatable with routine cleanings and improved hygiene, whereas advanced disease can cause tooth loss and systemic harm. We encourage all diabetic veterans to schedule a dental exam – both to protect their smile and to aid diabetes management. At Sayyar Family Dentistry in Glen Allen, our team is experienced in coordinating with your medical providers. We offer patient-focused care, modern techniques (including same-day CEREC crowns and preventative therapies), and convenient scheduling.
To make an appointment: Call (804) 290-8001 (See Contact info on our site). You can also [book an appointment online] at our Glen Allen office. Dr. Sayyar and staff look forward to helping Petersburg and Glen Allen veterans maintain healthy gums and overall health. Remember: controlling diabetes goes hand-in-hand with caring for your teeth.
Frequently Asked Questions
- Q: Why does diabetes cause gum disease?
A: High blood sugar weakens the gums’ defenses and blood supply. Diabetics make less saliva and have “glucose-rich” saliva, so more plaque forms. Their immune cells also work less effectively. All this makes infection more likely. Uncontrolled diabetes is often called a “complication” when gum disease develops. - Q: Can treating gum disease help my diabetes?
A: Yes. Studies show that deep cleaning (scaling/root planing) and good oral hygiene in diabetics often improve blood sugar control (lower HbA1c) for several months. It breaks the cycle of infection and inflammation. You will still need to manage diabetes medically, but tackling periodontal infection can make it easier. - Q: How often should a diabetic veteran see a dentist?
A: At least every 6 months is advised for routine care, but many diabetics need visits every 3–4 months. If you have active gum disease or loose teeth, your dentist may ask to see you more often to control the infection. - Q: What oral symptoms should raise concern?
A: Watch for persistent red/swollen or bleeding gums, loose teeth, new gaps between teeth, and ongoing bad breath. Dry mouth is also a warning sign (check for thick saliva or tongue soreness). If any of these occur, call your dentist immediately rather than waiting. Early intervention can prevent tooth loss. - Q: What help is available locally for veterans?
A: Eligible veterans may receive dental care through the VA dental program (e.g. McGuire VAMC) or through VA dental benefit expansions. Petersburg and Glen Allen residents can use local clinics like Southside Dental Cares or United Smiles (multiple offices) for general care. Free and low-cost options include Goochland Cares or Lucy Corr clinic. Dr. Sayyar’s practice welcomes veterans at our Glen Allen office (we coordinate with VA benefits and other providers). Call or check our [Contact page] to explore scheduling. - Q: Is tooth extraction safe if I have uncontrolled diabetes?
A: Diabetics can get extractions, but extra care is needed. High blood sugar should ideally be improved first, since healing is slower in uncontrolled diabetes. If you need a dental surgery, inform your dentist and physician. They may recommend extra antibiotics or schedule it after your sugar is better managed. Don’t avoid care – just communicate clearly with your care team.
Call (804) 290-8001 or contact Sayyar Family Dentistry for expert dental care. We serve Petersburg and Glen Allen, and look forward to helping you keep your gums healthy as part of your diabetes care.
Sources: Evidence-based clinical research and VA/public health data were used, including ADA/VA materials, systematic reviews, and local health resources. These inform our recommendations.