
Gum Disease Risk Factors in Veterans: Risks and Preventive Measures
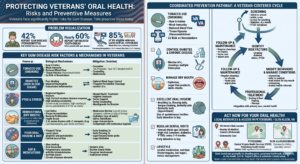
Executive Summary: Gum disease (periodontitis) is a chronic inflammatory infection that attacks the gums and tooth-supporting tissues. Veterans are at especially high risk due to common factors like smoking, diabetes, stress/PTSD, medication-induced dry mouth, and limited access to dental care. About 42% of veterans report gum disease, far above non-veterans, and nearly 60% report tooth decay. Contributing factors include a historically higher smoking rate in veteran populations (though this has declined to ~13.3% among VA enrollees as of 2020), a high prevalence of diabetes (~25% of VA patients), post-traumatic stress disorder (PTSD) and other mental health issues (affecting ~14% of male VA users), and multiple medications causing dry mouth. Smoking is a potent risk factor – smokers have roughly twice the gum disease risk of nonsmokers. Dry mouth (xerostomia), common in older veterans on multiple medications, reduces protective saliva and fosters plaque. Diabetes greatly exacerbates periodontal infection and healing. Moreover, PTSD and stress often lead to neglect of oral hygiene, compounding risk. These factors interact: for example, veterans with PTSD often smoke more and have worse hygiene.
Preventive strategies focus on risk modification and regular care. Veterans should be counseled on smoking cessation (using VA programs like Quit VET), optimal diabetes control (with more frequent dental cleanings), and managing dry mouth (hydration, saliva substitutes, and reviewing medications). Universal oral hygiene is critical: daily brushing/flossing and routine dental check-ups (at least yearly) are recommended. Community resources, such as Petersburg’s CVHS Health Center (which offers dental services) and VA dental clinics (locatable via the VA Dental Clinic Finder), can improve access. A coordinated prevention pathway (screening → risk modification → treatment → follow-up) is advised (see flowchart below). Clinicians should integrate these measures and consider veterans’ unique psychosocial context (e.g. anxiety that may deter care).
In Petersburg and Glen Allen, VA, local clinics and VA resources are available to veterans. Call or make an appointment for an oral exam if you have risk factors or symptoms (bleeding gums, loose teeth, dry mouth, etc.). Early intervention and lifestyle changes (smoking cessation, good oral hygiene, hydration, diabetes control) can halt or reverse gum disease. Call Dr. Sayyar’s office to schedule a dental exam, especially if you are a veteran experiencing gum problems.
| Risk Factor | Prevalence (Veterans) | Biological Mechanism | Mitigation |
| Tobacco Use (Smoking) | ~13.3% of VA-enrolled veterans smoke (2020); many more are ex-smokers. | Smoke irritates gums, weakens immune response and blood flow, and fosters plaque. Smokers have ~2× risk of periodontitis. | Quit smoking using VA cessation programs; nicotine replacement; counseling and medications. Dental professionals should note smoking history and reinforce quitting. |
| Diabetes (High blood sugar) | Affects ~25% of VA patients. | Diabetes impairs neutrophil function and increases inflammation in gums, making infections worse and healing slower. Periodontal infection can also worsen glycemic control (bidirectional link). | Strict glycemic control (monitor A1c) and smoking cessation. More frequent periodontal cleanings and blood sugar management recommended. |
| Psychological Stress/PTSD | PTSD in ~14% of male VA patients (2024 data); higher in female veterans. | PTSD/anxiety often leads to neglected oral hygiene and bruxism. Stress hormones may impair immunity, increasing susceptibility to gum infection. Veterans with PTSD on meds smoked more and had 62% severe periodontitis (vs ~15–30% in others). | Mental health treatment and social support, dental counseling. Emphasize routine hygiene. Smoke cessation is key if smoking co-occurs. Consider dental inserts (mouthguards) if bruxism is present. |
| Xerostomia (Dry Mouth) | Common in older veterans; est. 30–40% of adults >65 report dry mouth. Veterans often take multiple meds causing dryness. | Reduced saliva allows plaque accumulation and oral bacteria to thrive. Dry mucosa is prone to cracks and infection. Many xerogenic meds (antidepressants, antihypertensives, diuretics, etc.) have anticholinergic effects. | Review medications (may switch to less xerogenic options or adjust timing). Encourage frequent sips of water, sugar-free gum/lozenges, saliva substitutes. Avoid alcohol and caffeine. Maintain meticulous hygiene to compensate for reduced saliva. |
| Poor Oral Hygiene & Diet | Survey data: >40% of adults had mouth pain in last year. Veterans’ oral care practices vary widely. | Inadequate brushing/flossing allows plaque (bacterial film) to mineralize into tartar, directly causing gingivitis and periodontitis. High sugar intake fuels bacteria. Limited access/dental fear can worsen self-care. | Daily brushing (2×) and flossing (1×) are non-negotiable. Use fluoride toothpaste and plaque-disclosing tools if needed. Limit sugary snacks. Dental professionals should educate veterans on technique and provide encouragement (and products). |
| Age & Medications | Majority of veterans are older; many take 4+ daily meds. | Aging by itself causes gum recession and slower healing. Polypharmacy increases xerostomia and nutritional issues. Chronic diseases (arthritis, vision loss) can limit care ability. | Geriatric-focused oral care aids (flossers, electric brushes). Ensure caregivers/clinicians assist if needed. Regular dental visits are critical for seniors. Encourage caregivers’ involvement and coordinate with primary care for med review. |

Veterans and Gum Disease: Periodontitis is markedly more prevalent in veterans than the general population. A recent report found 42% of veterans self-reported having gum disease, likely reflecting both high risk factors and limited access to care (85% of VA-eligible veterans lack dental coverage). Additionally, 60% of veterans reported untreated tooth decay, often coexisting with periodontal disease. Local demographics show Petersburg’s population is ~9.5% veteran and Glen Allen’s ~6.7%, so many local residents are at risk.
Notably, smoking remains a dominant risk. Although veteran smoking rates have declined, in 2020 about 13.3% of VA patients were current smokers (similar to the U.S. average of ~14%). Smoking impacts periodontium by vasoconstriction, immune suppression, and tissue hypoxia, making gum infections more aggressive. The CDC emphasizes that “you have twice the risk for gum disease compared with a nonsmoker”, and that smoking reduces treatment success and healing. In veterans, cultural factors and PTSD have historically led to higher smoking rates; a study of PTSD-affected veterans showed those on psychiatric meds smoked far more and had 62.5% prevalence of severe periodontitis vs ~15–30% in others.
Diabetes is another key factor. Nearly one-quarter of VA patients have diabetes, often Type 2 related to age or Agent Orange exposure. Chronically high blood glucose impairs neutrophil function and increases gum inflammation. The VA explicitly warns that “You may be at greater risk for gum disease when you have diabetes”, and advises tight glycemic control to mitigate this risk. Conversely, untreated periodontitis can worsen diabetes control, making dental health part of overall chronic disease management.
PTSD and mental health issues are widespread in veterans and indirectly raise gum disease risk. Veterans with combat-related PTSD often neglect routine care due to depression/anxiety or dental phobia. Research shows PTSD patients have poor oral hygiene, rampant cavities, missing teeth, and more severe periodontal disease. For instance, an Israeli study found every combat-veteran with PTSD had poor dental status, and among those on psychiatric medications 62.5% had severe periodontitis (versus 27% in controls). The authors attributed this to “neglected oral hygiene, decreased natural immunity, and smoking habits” in PTSD patients. Even aside from PTSD, military service stressors and shift work can disrupt self-care habits.
Dry mouth (xerostomia) is highly relevant in veterans, especially older ones on multiple drugs. The ADA notes dry mouth affects ~30% of people over 65, and veterans often take medications with strong xerogenic (saliva-reducing) effects (antidepressants, anticholinergics, antihypertensives, pain meds). A VA study found that veterans on even one xerostomic medication were ~2.6× more likely to have severely dry oral mucosa than those on none. With low saliva, plaque removal is compromised and mucosal defenses are weakened. Dryness encourages caries and can exacerbate gingival inflammation (though one study found no direct increase in periodontal score, dry tissue itself is more fragile). Clinically, xerostomia in veterans may arise from PTSD meds, pain killers (including opioids), or radiation/cancer treatments.
Other factors include age and sex: most veterans are older males, who naturally have some receding gums and slower healing, and often multiple health conditions. Aging per se causes reduced salivary flow (e.g. nursing home studies show up to 40% of >80-year-olds have dry mouth) and limitations in dexterity. Genetic susceptibility also plays a role – some individuals inherently react to plaque with more inflammation (though genetic risk is hard to quantify clinically). Poor diet and nutrition (high sugar intake, low fruit/veggies) common in any population will similarly affect veterans. Finally, access to care is a systemic factor: since 85% of VA-enrolled veterans lack dental benefits, many delay care until disease is advanced. This lack of preventive care magnifies all other risks.
Smoking and Veterans’ Oral Health
Tobacco use is a dominant preventable risk. In veterans, smoking often coexists with other risk factors (PTSD, diabetes, low socioeconomic status). As a result, 60–85% of periodontitis cases in some studies are attributable to smoking. Mechanistically, nicotine and other smoke components cause blood vessel constriction and immunosuppression in the gums, so infections flourish. The CDC notes: “Smoking is an important cause of severe gum disease in the United States”, and clearly states smokers “have twice the risk for gum disease compared with a nonsmoker”. Moreover, tobacco impairs gingival healing – smokers respond poorly to periodontal therapy.
For local veterans, quitting smoking should be a top priority. The VA runs strong tobacco-cessation programs: e.g. Quit VET (phone counseling 1-855-QUIT-VET) and SmokefreeVET texting service. These should be integrated into dental visits – dental clinicians can refer patients to these services. Even modest reductions in smoking (fewer cigarettes per day) can lower gum disease risk. On the positive side, the overall veteran smoking rate is falling: VA reports show enrollment smoking prevalence dropped from 33% (1999) to 13.3% (2020). Encouragement and nicotine-replacement therapies should be offered to any veteran smoker.
Smoking mitigation: Stop all tobacco use (including cigars, pipes, chew); participate in VA smoking-cessation programs. Dental providers should note smoking history, reinforce risks, and schedule more frequent cleanings for smokers. Quitting not only reduces gum disease risk but also improves diabetes control and cardiovascular health.
Dry Mouth (Xerostomia) in Veterans
Xerostomia (chronic dry mouth) is highly prevalent in elderly and medicated populations. Among veterans it’s common because many take multiple prescriptions (for hypertension, PTSD, pain, etc.) that reduce saliva. When saliva production drops, the mouth’s natural cleansing and buffering abilities are compromised. Plaque and food debris linger, pH drops, and bacteria proliferate, raising the risk of both tooth decay and gum infections. A study of New England VA patients found those on ≥1 xerogenic drug were 2.6 times more likely to have severely dry oral tissues.
Veteran examples: An older veteran on antidepressants and antihypertensives may wake with a dry, burning mouth every morning. Over time, he might notice increased gingival inflammation or cavities. Without enough saliva, flossing is painful, so hygiene falters. In clinics, many VA dentists encounter veterans complaining of sticky saliva or cracked lips.
Contributing factors: The ADA explains that over 100 medications (especially antidepressants like SSRIs, antipsychotics, and anticholinergic drugs) have strong evidence of causing salivary gland dysfunction. Veterans may also have dryness from radiation therapy (if they had head/neck cancer) or even chronic dehydration.
Mitigation: The first step is medical review. Clinicians should ask about dry mouth and review the veteran’s medications. If possible, some drugs can be substituted. For example, switching a tricyclic antidepressant to an SSRI may lessen dryness. Changing medication timing (taking dry-mouth-inducing meds at night) or splitting doses can help. If meds cannot be changed, symptomatic relief is key: drink water regularly, chew sugar-free gum or suck on xylitol lozenges to stimulate saliva, and consider over-the-counter saliva substitutes. Dentists may recommend prescription mouth rinses or topical fluoride to protect teeth.
Moreover, maintain excellent oral hygiene: brushing twice daily with fluoride toothpaste, flossing daily, and using a soft-bristled brush to avoid gum trauma. Hydration is vital – veterans should be counseled to sip water frequently, especially when taking xerogenic meds. Avoid alcohol, caffeine, and spicy foods that can worsen dryness. If lab tests suggest severe hyposalivation (e.g., after radiation), medications like pilocarpine (a sialogogue) may be considered (VA formulary).
In summary, dry mouth in veterans often arises from their medication load and age, and can significantly contribute to gum disease if unaddressed. Proactive measures – medical adjustment, saliva stimulation, frequent dental cleanings – can counteract this risk factor.
Other Risk Factors
- Diabetes: As noted, poorly controlled diabetes can double or triple the risk of periodontitis, and infections heal poorly. Every veteran with diabetes should be flagged for periodontal assessment. Dentists should work with patients’ physicians to manage blood sugar; coordinated care (e.g. at a VA diabetes clinic) is ideal.
- Poor Oral Hygiene: Beyond patient-driven factors above, some veterans face barriers to hygiene: disabilities from war injuries, vision loss, or limited income for dental supplies. Education and assistance (e.g., superflossers, water picks) are important.
- Nutrition: Excessive sugar or frequent snacking without oral care promotes plaque. Dentists should counsel veterans on diet (limiting sodas, candy) and emphasize that gum disease prevention is not just brushing – it’s also about eating well.
- Genetics/Immune Status: Some individuals genetically mount a stronger inflammatory response to plaque. While non-modifiable, dentists can identify these patients by observing rapid periodontal breakdown and intensify treatment (e.g. scaling every 3 months).
- Access to Care: Although not a “biological” risk factor, lack of routine care is a key driver of severity. Only 15% of VA patients have dental coverage, so many veterans delay dental visits until pain or advanced disease. Local VA clinics (if qualified for certain illnesses, like SC disability or head/neck cancer) can offer prosthodontics or limited care. It’s crucial to connect veterans with community resources: for example, the Petersburg Central Virginia Health Services (CVHS) Health Center provides dental care regardless of insurance. Clinicians should ask about coverage and refer uninsured veterans to community clinics or local dental missions. In Petersburg, the VA locator and CVHS clinic are critical resources.
Preventive Measures and Oral Hygiene
Preventing gum disease requires a multi-pronged approach. The CDC outlines broad prevention tips that apply to veterans:
- Quit Tobacco: As above, stopping smoking (and all tobacco) is paramount. Smoking cessation not only cuts gum risk, but also reduces cancer and heart disease in veterans.
- Control Diabetes & Chronic Disease: Keeping A1c and blood pressure in targets helps the gums heal. CDC advises diabetics to get dental cleanings multiple times per year. Veterans should be reminded that oral health is part of diabetes care.
- Manage Dry Mouth: Drink water, chew gum, and discuss medication timing to prevent hyposalivation. Avoid bedtime doses of xerogenic drugs if possible.
- Excellent Oral Hygiene: Brushing twice daily and flossing daily remove plaque before it hardens into tartar. Veterans with dexterity issues can use electric toothbrushes or floss holders. Cleaning the tongue can also reduce bacterial load.
- Regular Dental Visits: The CDC recommends at least annual check-ups. For high-risk veterans (smokers, diabetics, PTSD), even more frequent cleanings (every 3-4 months) may be needed. These visits allow early detection of gingivitis. Dr. Sayyar’s office in Petersburg offers comprehensive exams and cleanings – veterans should be encouraged to use these services. (For immediate issues like severe pain or swelling, emergency dentistry is available.)
- Fluoride and Sealants: While cavity prevention is often separate, fluoride use (toothpaste, rinses, fluoridated water) also protects tooth roots exposed by receding gums. The cavity prevention page has tips relevant to all patients. In some cases, dentists may apply topical fluoride or sealants to vulnerable teeth or roots.
- Lifestyle: Beyond smoking, alcohol moderation is wise – heavy drinking is another risk. Adequate nutrition (fruits, vegetables, low sugar) supports tissue health. Stress management (exercise, therapy) may indirectly benefit oral health by improving self-care.
Mermaid Flowchart – Prevention Pathway: The prevention process can be visualized as a cycle:
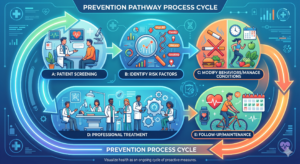
– Screening: Any veteran (especially at initial visit or annual exam) should be screened for smoking status, diabetes history, dry mouth, and PTSD symptoms. Dental x-rays and periodontal probing help detect early disease.
– Risk Modification: Based on findings, counsel on quitting, refer to medical care, adjust meds for dry mouth, etc.
– Treatment: For existing gum disease, perform scaling/root planing and other appropriate therapy.
– Follow-Up: Schedule re-checks. Reinforce home care at each visit and adjust plan as needed.
The CDC emphasizes that these measures work together: “Good oral health means good overall health”. Clinicians should integrate oral care into veterans’ medical care – for example, primary care providers reminding diabetic patients about flossing, or mental health providers encouraging PTSD patients to keep dental appointments.
Local Resources and Access (Petersburg/Glen Allen, VA)
Veterans in Petersburg and Glen Allen have access to both VA and community dental services. The VA website provides a Dental Clinic Locator tool to find VA-approved clinics. While Petersburg has no full VA dental hospital, nearby VA Medical Centers (Richmond) and Community Care programs can often provide basic services. Importantly, Central Virginia Health Services (CVHS) Petersburg Health Center offers dental care regardless of income or insurance. Their dental department can see veterans who lack coverage or need sliding-scale care. In Glen Allen/Richmond, several community health centers and dental practices (including specialty clinics) serve veterans.
Call to Action: Veterans are urged to proactively address oral health. If you notice bleeding gums, persistent bad breath, gum recession, loose teeth, or dry mouth, schedule a dental exam immediately. Prevention and early treatment are far easier than dealing with advanced disease. Dr. Sayyar’s practice in the Petersburg area provides expert periodontal care – call or use our Contacts page to make an appointment. We also serve families: veterans with children can benefit from our pediatric dentistry services to instill good habits early. For sudden dental pain or injury, emergency dentistry is available 24/7.
In summary, veterans face several modifiable and non-modifiable risk factors for gum disease. By combining evidence-based prevention (smoking cessation, hydration, hygiene, professional care) with awareness of veteran-specific issues (PTSD, medications, access barriers), both patients and clinicians can dramatically reduce the burden of gum disease. Get screened and start prevention today – early action preserves your teeth, health, and well-being.
FAQs (Frequently Asked Questions)
Q: Are veterans more prone to gum disease than civilians?
A: Yes. Studies show veterans have higher rates of dental issues: about 42% report gum disease (versus ~28% in the general adult population). Factors include more smoking, diabetes, PTSD, and often less dental coverage. Veterans’ unique health profiles (e.g. military exposures) can also contribute.
Q: How does smoking affect a veteran’s gums?
A: Smoking significantly worsens gum health. It reduces blood flow and immunity in gums, making infections more severe. Smokers have roughly twice the risk of periodontitis compared to non-smokers. Quitting smoking is the single most impactful change a veteran can make to protect gums. VA offers free quitting programs and medication to help veterans stop smoking.
Q: What causes dry mouth (xerostomia) in veterans?
A: Many veterans take medications (antidepressants, blood pressure drugs, pain meds, etc.) that have side effects of reduced saliva. Older age and conditions like diabetes also contribute. Dry mouth means less natural cleansing of the mouth, so plaque builds up more easily. To manage it, veterans should stay hydrated, use saliva substitutes (like artificial saliva sprays), chew sugarless gum, and talk to their doctor about adjusting medications if possible.
Q: How can veterans prevent gum disease?
A: Prevention involves multiple steps. First, maintain excellent daily oral hygiene: brush twice with fluoride toothpaste and floss daily to remove plaque. Quit tobacco and limit alcohol. Control systemic health: manage diabetes (good blood sugar control) and other conditions. Stay hydrated and address dry mouth (water, sugar-free gum). Visit the dentist regularly (at least once a year, or more often if you have risk factors). Professional cleanings and exams can catch gum inflammation early. Using these measures together – as recommended by the CDC – greatly reduces gum disease risk.
Q: What should I do if I’m a veteran in Petersburg/Glen Allen with gum problems?
A: Seek dental care promptly. Petersburg’s CVHS Health Center has dental services for veterans. You can also contact Dr. Sayyar’s office for an evaluation. If you have severe symptoms (swelling, abscess, or trauma), use our emergency dentistry services immediately. Otherwise, schedule a check-up to discuss prevention and treatment. Even without VA dental benefits, community clinics and sliding-scale programs can assist veterans in the area.