
Periodontal Treatment Options in Petersburg & Glen Allen, VA: Non‑Surgical Therapy vs Surgery
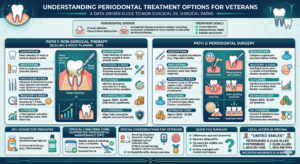
Executive Summary: Veterans with gum disease have two main treatment paths: non-surgical therapy (deep cleaning/scaling and root planing plus possible antibiotics and maintenance) and surgical procedures (flap surgery, osseous resection, grafting, etc.). Non‑surgical therapy is first-line for mild-to-moderate periodontitis and can significantly reduce pocket depths and inflammation. If disease is advanced (deep pockets ≥6 mm, bone loss, or failed response to cleanings), surgery may be needed to gain access and regenerate tissue. Clinical evidence shows surgery achieves greater pocket reduction in deep sites, but long-term attachment levels are similar. Both approaches require patient factors (smoking, diabetes, PTSD, etc.) to be managed for best outcomes. For veterans, many qualify for VA dental coverage (Class I/II), making needed periodontal care affordable. Local clinics (e.g. United Smiles Petersburg or Glen Allen) offer these services; call (804) 894‑9393 for Petersburg or (804) 999‑9099 for Glen Allen.
Understanding Periodontal Disease and Treatment Goals
Periodontitis (“gum disease”) is chronic infection that destroys the tissues and bone supporting teeth. It starts as gingivitis (red, bleeding gums) and can progress silently. Risk factors include poor oral hygiene, smoking, diabetes, and genetics. Untreated, it leads to loose teeth and tooth loss. Both non-surgical and surgical treatments aim to arrest infection, reduce pocket depths, and rebuild healthy attachment. The initial goal is to remove plaque and calculus (biofilm and tartar) to allow healing. Non-surgical therapy (scaling and root planing, SRP) removes subgingival bacteria and toxins. If pockets remain deep or bone defects persist, surgical therapy (flap access, osseous reshaping, regenerative procedures) follows. Both paths require ongoing supportive therapy (periodontal maintenance) to prevent relapse.
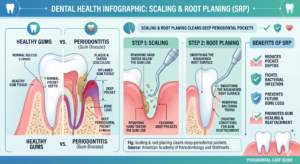
Non‑Surgical Periodontal Therapy (Scaling & Root Planing)
- Description: Deep cleaning of root surfaces to remove plaque, calculus and bacterial toxins. Often called “deep cleaning.”
- Indications: Mild to moderate periodontitis (pockets ≤5 mm), or the first stage of treatment for severe disease. Also used to reduce inflammation before any surgery.
- Procedure Steps: Performed quadrant-by-quadrant. With local anesthetic, ultrasonic scalers and hand instruments “scale” (remove deposits) and “plane” (smooth roots) to eliminate bacteria and roughness. May be done over 1–4 visits. Hygienist or periodontist instructs improved oral hygiene. Adjuncts like chlorhexidine rinses or delivered antimicrobials may be used.
- Anesthesia: Local anesthesia (e.g. lidocaine with epinephrine) is typically used for patient comfort. Nitrous or sedation is optional for anxious veterans.
- Recovery: Patients may have tenderness and minor bleeding for 1–3 days. No stitches are involved. Oral hygiene continues normally. Sensitivity to cold may occur as roots are exposed. Most return to work immediately. A re-evaluation occurs ~6–8 weeks later.
- Risks/Complications: Post-procedure sensitivity and minor discomfort. Gum recession may be noted as inflammation resolves. Rarely, infection (abscess) can occur. SRP itself has low risk. Poor outcomes are more likely if patients smoke or have uncontrolled diabetes.
- Outcomes/Prognosis: SRP typically reduces probing depths by ~1–3 mm in moderate pockets and reattaches gum to tooth. AAP/ADA guidelines state SRP has “moderate benefit” and is recommended as initial therapy for chronic periodontitis. Most improvement is seen in the first 3–6 months, and many sites heal fully. Ongoing maintenance is needed to sustain gains.
- Typical Cost Range: About $200–$300 per quadrant (4 quadrants full mouth), so ~$800–$1,200 total. (Costs vary by provider and insurance.) Many dental plans and VA benefits can reduce this.
- VA Coverage/Benefits: For eligible vets (see below), SRP is “needed dental care” and covered. Even those in Class IIA (service-related noncompensable) qualify if it’s needed to maintain a functional dentition. Veterans without VA dental benefits may use dental insurance/VADIP.
- Suitability (Comorbidities): SRP is safe for most. Patients with diabetes should aim for good glycemic control before treatment. Smokers should be advised to quit to improve healing. PTSD/anxiety veterans may benefit from sedation options during SRP.
Adjunctive Therapies and Maintenance
- Adjunctive Antibiotics: In certain cases, systemic or local antibiotics are used with SRP. ADA guidelines strongly recommend sub-antimicrobial dose doxycycline for chronic periodontitis adjunctively. Full-dose antibiotics (e.g. metronidazole + amoxicillin) yield extra benefit but have more side effects (so guideline gives weak recommendation). Other adjuncts (e.g. chlorhexidine chips) have weak evidence.
- Antimicrobial Mouth Rinses: Chlorhexidine or essential oil rinses can help reduce bacteria post-SRP. These are conservative, low-risk measures used early in treatment (also mentioned by local practices).
- Supportive Periodontal Therapy (Maintenance): After active treatment (surgical or not), regular maintenance is critical. Usually every 3–6 months, patients undergo exams and prophylaxis to prevent recurrence. StatPearls notes most patients require ongoing maintenance therapy after SRP. Evidence supports frequent recall reduces tooth loss in periodontitis patients. Indication: All periodontitis patients, especially smokers and diabetics. Recovery/Procedure: Professional cleaning with or without local antimicrobials. Outcomes: Maintains pockets and prevents progression. Cost: Varies (often covered by insurance/dental plans). VA covers maintenance as ongoing care if in benefit class. Suitability: Essential for all.
Periodontal Surgery Options
When non-surgical therapy cannot fully control disease (deep pockets, persistent inflammation, or complicated anatomy), periodontal surgery is indicated. Surgical options improve access to root surfaces and allow reshaping of bone and gums to reduce pockets. Key surgical procedures include:
Flap Surgery (Pocket Reduction / Access Flap)
- Description: The gums are carefully incised and lifted (flap) to expose roots and bone. Root surfaces are then debrided thoroughly. In access/pocket reduction surgery (often combined with osseous surgery), the flap is sutured back with reduced pocket depth. Apically positioned flaps (root repositioned) can further decrease pocket depth.
- Indications: Persistent deep pockets (≥6 mm) after initial therapy; inability to fully clean subgingivally with non-surgical means; greater site-specific bleeding or bone defects.
- Procedure Steps: Under local anesthesia, incisions (e.g. Modified Widman or apically positioned) are made to reflect a full-thickness flap. Granulation tissue and calculus are removed from roots. For pocket reduction, the flap is re-sutured at a new position (often more apical). If combined with osseous resection (see below), bone may be contoured. Flap design depends on defect and esthetics. Sutures are placed to adapt tissue.
- Anesthesia: Local anesthesia is standard; nitrous or sedation may be offered. Pain management may include long-acting anesthetic (bupivacaine) and NSAIDs. Antibiotics are not routinely needed unless indicated (e.g., penicillin for penicillin-allergic patients or complicated cases).
- Recovery: Expect surgical swelling and discomfort for ~1–2 weeks. Diet soft foods initially. Rinsing with chlorhexidine and careful hygiene around the site. Stitches are typically removed after 1–2 weeks. Full comfort returns as tissues heal (often within 2–4 weeks). Compared to extractions, flap surgery has less intense pain and quicker recovery since tissue is repositioned for primary healing.
- Risks/Complications: Bleeding, infection, post-op pain. Greater risk of gingival recession and tooth sensitivity (especially with osseous resection). If a flap is apically positioned, the crown appears longer. Care must be taken near nerve or aesthetic areas. Smoking or systemic issues (diabetes, immunosuppression) increase complications.
- Outcomes/Prognosis: Flap surgery typically yields significant reduction in deep pocket depths (>4 mm) and gains in attachment. For example, osseous flap procedures often achieve >2 mm PD reduction in deep sites. However, increased recession is a trade-off. Systematic reviews show surgical therapy provides greater pocket depth reduction in deep pockets than SRP alone. Long-term (5+ years), surgical pockets remain shallower (about 0.5 mm more gain for >7 mm pockets), but clinical attachment gains tend to be similar between approaches.
- Typical Cost Range: Surgical pocket reduction averages about $500–$1,200 per quadrant (higher than SRP). Costs vary widely by clinic and complexity.
- VA Coverage: For eligible veterans, periodontal surgery is “needed dental care” and covered under Class I/II benefits, similar to SRP. The VA often requires referral to a VA or contracted dentist.
- Suitability (Comorbidities): Flap surgery can be performed in older patients and those with controlled chronic conditions. Special considerations: Smokers should quit to improve healing; diabetics must have good glucose control; PTSD/anxiety may need sedation. Contraindications: Poor oral hygiene or unwillingness to maintain therapy; uncontrolled systemic disease may delay treatment.
Osseous Resection (Bone-Contouring)
- Description: Often done with flap surgery, osseous resection involves surgically reshaping the jawbone to a more favorable architecture. Bone shelves and defect walls are removed to create a positive (physiologic) bone form. This reduces pocket depth by eliminating deep bony craters.
- Indications: Shallow to moderate vertical bone defects in posterior sites; multirooted teeth with wide pockets. Generally used when intrabony defects are shallow (<3 mm). Also used for crown lengthening (below).
- Steps: After raising the flap, bone is cut with burs or hand instruments. The goal is to reduce bone peaks and create a flat or gently scalloped architecture. Affected root surfaces are exposed to less pocket depth. The flap is then sutured in place, often more apically.
- Anesthesia: As above (local anesthetic, etc.). Patients may receive post-op antibiotics if large bone removal or graft placement is done.
- Recovery: Similar to flap surgery. Some extra soreness due to bone work. 1–2 week healing for soft tissue, with sensitivity possible. Ibuprofen and ice packs help.
- Risks: More tooth sensitivity (dentin exposure), gingival recession. If esthetic areas, careful planning needed. Over-resection can compromise tooth stability.
- Outcomes: Excellent pocket reduction (often 3–4 mm gain in moderate pockets). Bone resection permanently reshapes the site, so pockets remain closed long-term. Attachment levels stabilize to bone level.
- Cost: Bone resection is part of flap surgery, so costs combined. Standalone osseous surgery (e.g. 1 quadrant) ~$800–$1,200.
- VA Coverage: Covered as needed care.
- Comorbidities: Same cautions as flap surgery. Radiation therapy or bisphosphonates increase risk of osteonecrosis (rare in jaw surgery) – need physician consult.
Bone Grafts & Guided Tissue Regeneration (GTR)
- Description: Regenerative surgery uses graft materials and barrier membranes to regrow lost bone and tissue. Materials include autograft (patient’s bone), allograft (donor bone), xenograft (animal), or alloplast (synthetic). Guided Tissue Regeneration uses a membrane over the graft to direct healing. The goal is new bone, periodontal ligament, and cementum formation.
- Indications: Deep vertical (intrabony) defects ≥4 mm and 2–3 wall morphology; grade I-II furcation lesions; implant site preservation. Typically after initial therapy, in sites with “good regenerative potential”.
- Steps: Flap is raised; defect is debrided. Biologics (e.g. enamel matrix derivative, growth factors) may be applied. Graft particles are packed into the bone defect. A resorbable or non-resorbable membrane covers the area. Flap is sutured tightly to exclude epithelium. (See e.g. Box technique in ).
- Anesthesia: Local anesthesia as usual. Post-op antibiotics (e.g. amoxicillin) are common in grafting/GTR surgeries to prevent infection, though optimal regimen is debated. Pain control and steroids (dexamethasone) may be prescribed for swelling.
- Recovery: Longer healing. Soft tissue takes ~2 weeks; bone regeneration continues over months. Patients have strict oral hygiene and usually avoid flossing/burshing at site initially. Follow-up visits to remove sutures and check healing.
- Risks: Infection risk at graft site; membrane exposure (if flap fails to seal); unpredictable bone fill if patient is a smoker or diabetic. Pain and swelling may be more pronounced due to graft and membrane.
- Outcomes: When successful, bone graft/GTR can fill defects and gain clinical attachment. Systematic reviews show significant pocket reduction (~4–5 mm) and bone fill in favorable cases. However, results vary by defect type. A Cochrane review notes GTR improves bone level vs flap alone in deep defects. Patients with controlled conditions see the best results.
- Cost: Very variable. Bone grafting can range $500–$2,000 or more per site (depending on graft type). GTR membrane adds cost (~$300–$1,000). The statpearls page [25†L188-L197] cites graft costs $549–$5,148 by type.
- VA Coverage: Covered if case qualifies as needed to save tooth and function. VA may require demonstration of medical necessity (i.e., damage from periodontitis).
- Comorbidities: Higher failure risk if smoking or uncontrolled diabetes. These patients need careful control. PTSD/anxiety can make compliance with post-op care difficult, so counseling and support are important.
Crown Lengthening
- Description: Surgical removal of gum (and sometimes bone) to expose more tooth structure. Used to make restorations possible or improve appearance. In periodontics, it often involves an apically positioned flap with osseous resection to create a biologic width.
- Indications: Subgingival decay or fracture below the gum line; inadequate ferrule for a crown; “gummy smile” (altered passive eruption) correction. It is not a treatment for infection per se, but used to save/restorability of a tooth.
- Steps: Full-thickness flap is made, bone is removed around the tooth so that 4+ mm of sound tooth is exposed above the bone. Flap is sutured lower on the tooth. Healing creates longer-looking tooth.
- Anesthesia: Local anesthesia (often includes nerve block plus infiltration). Sedation optional. Pain meds (NSAIDs) and sometimes antibiotics.
- Recovery: Similar to flap surgery above; expect 1–2 weeks of soft-tissue healing. Temporary crowns/provisional restorations must stay in place for a few weeks during healing.
- Risks: Gingival recession around treated and adjacent teeth; sensitivity; root caries risk. Overzealous bone removal can compromise future implant placement.
- Outcomes: Restores adequate tooth height for restorative work. When done properly, results are stable. Studies report ~2–3 mm of additional clinical crown length on average. Patients report easier hygiene around crowned teeth.
- Cost: ~$500–$3,000 per tooth depending on complexity (one tooth vs multiple).
- VA Coverage: Considered “necessary dental care” if to save a functioning tooth.
- Suitability: Patients must understand the esthetic change (teeth will look longer). Smokers and diabetics heal more slowly. Not done if it would expose a furcation or if it would make future implants impossible.
Dental Implants (Tooth Replacement)
- Description: Titanium posts surgically placed to replace tooth roots, topped with crowns. Indicated when teeth are lost to periodontitis. While not a periodontal procedure, implants are often discussed when periodontal treatment fails or teeth must be extracted.
- Indications: Missing teeth with adequate bone or after bone grafting; patient desires fixed replacement; good overall health. Careful if patient has active periodontal disease (periodontitis must be controlled first).
- Steps: Extraction (if needed) and bone grafting (if deficient). After healing (2–6 months), implant placement under local anesthesia. Usually 3–6 months osseointegration, then second stage to attach an abutment and crown.
- Anesthesia: Local anesthesia (often plus sedation for comfort). Post-op pain managed with NSAIDs. Antibiotics are typically given for 5–7 days post-surgery. Implants in medically compromised vets are carefully coordinated with physicians.
- Recovery: Initial healing ~1–2 weeks (soft tissue). Full bone integration takes months. Temporary diet modifications and antibiotics. Once healed, patient is restored with a permanent crown.
- Risks: Implant failure/infection (peri-implantitis), nerve injury, sinus issues in upper jaw. Smoking and diabetes significantly increase failure risk.
- Outcomes: High success rates (~90–95% at 5 years in healthy patients). Provide superior function compared to bridges/dentures. Periodontal health around implants requires maintenance akin to natural teeth.
- Cost: In Virginia, a single implant (post, abutment, crown) averages $3,000–$5,500. Additional bone grafting adds $400–$2,500. Overall full-mouth reconstruction can exceed $20,000.
- VA Coverage: Usually not covered under routine dental benefits (only for service-related traumatic dental injury). Veterans may use VA Dental Insurance or private insurance.
- Suitability: Not ideal for heavy smokers or poorly controlled diabetics (high failure). PTSD or seizure disorders require precaution (avoid sleep aids that could cause aspiration). Age alone is not a contraindication if health is OK.
Comparing Outcomes: Therapy vs Surgery
Clinical studies and guidelines emphasize a stepwise approach. Non-surgical therapy is the first step for all periodontitis cases. If deep pockets (>6 mm) remain, surgical options follow. Systematic reviews show that:
- Pocket Depth Reduction: Access flap surgery yields significantly greater PD reduction in deep sites than SRP alone. For pockets initially ≥7 mm, surgery may add ~0.5 mm of extra reduction even at 5-year follow-up. In moderate pockets (4–6 mm), surgery gives more reduction short-term, but differences vanish long-term. Overall, the deeper the defect, the more benefit from surgery.
- Clinical Attachment Gain: Meta-analyses (1990s) reported slightly more attachment gain with SRP in moderate pockets, possibly because shallow pockets “gain” more after non-surg. In deep pockets, surgery can achieve good attachment gain, but differences are small. By 5 years, attachment outcomes are generally similar between approaches.
- Healing and Stability: Surgical therapy provides direct vision to ensure complete debridement and can correct osseous defects that nonsurgical cannot. Long-term, teeth treated surgically with maintenance can remain stable. Nonsurgical therapy is highly effective for mild-to-moderate disease, especially if patients practice excellent hygiene.
- Adjunctive Benefits: Both therapies often require adjunctive maintenance (SRP maintenance or reentry flap) to sustain gains. Studies note that supportive periodontal therapy is critical regardless of initial method.
In summary, non-surgical therapy effectively controls early to moderate periodontitis and improves most sites. Surgery is reserved for sites where bacteria remain sheltered or bone defects persist; it produces greater pocket reduction in such cases. Both paths converge on the goal of a healthy, maintainable dentition. For veterans, early detection and treatment (via SRP) can often avoid surgery. But if surgery is needed, it remains a covered and effective option.
Special Considerations for Veterans
Veterans may have unique factors affecting periodontal care. Comorbidities: Smoking (higher in veteran populations) drastically impairs healing and is linked to persistent pockets. Diabetes (also common in older vets) increases infection risk and slows wound healing; glycemic control should be optimized before intensive therapy. PTSD or dental anxiety can make any dental procedure challenging; sedation dentistry or empathetic care can help. Medications (e.g. warfarin, bisphosphonates) require care (consult with medical providers).
VA Dental Benefits: The VA provides dental care only to eligible veterans. Key categories (Class I & II) get any needed care. Specifically: veterans with a service-connected dental disability, prisoners of war, or 100% disabled (Class I/IV) qualify for full dental benefits. Class IIA (noncompensable dental disability or combat injury) covers needed care to maintain a functional dentition. Many periodontitis treatments (SRP, surgery, maintenance) qualify as “needed care.” Those not enrolled in VA benefits can use the Veterans Dental Insurance Program (VADIP) or other insurance. Always verify current VA policy for dental eligibility.
Local Access in Petersburg/Glen Allen: Veterans in Petersburg or Glen Allen can access periodontal therapy at VA clinics (if available) or local practices. For example, United Smiles has offices in Petersburg (34 E. Medical Park Blvd, Petersburg) and Glen Allen (5332 Wyndham Forest Dr) offering scaling, surgical therapy, and implants. These offices accept new patients and many insurance plans. Call (804) 894‑9393 for Petersburg or (804) 999‑9099 for Glen Allen to schedule an evaluation. (Or ask your primary care provider to refer you.) Early referral to a periodontist may be warranted for severe cases or complex needs.
Frequently Asked Questions (FAQ)
Q: What’s the difference between gum therapy (SRP) and periodontal surgery?
A: Scaling and root planing (non-surgical therapy) cleans the teeth below the gumline to remove infection. Periodontal surgery (flaps, grafts) is needed if deep pockets or bone defects remain after cleaning. Surgery allows the dentist to reshape bone and gum for better healing.
Q: How long is recovery after periodontal surgery?
A: Typically 1–2 weeks of initial recovery (swelling, tenderness). With proper pain management (NSAIDs) and rest, most discomfort subsides in a few days. Full tissue healing takes longer. SRP (non-surgical) has minimal downtime (usually just soreness a day or two).
Q: Will the VA cover gum disease treatment for me?
A: Possibly. Veterans in Classes I or II (service-connected disabilities, POW, or 100% disabled) get any needed dental care. Class IIA (service-connected but non-compensable) covers care to keep a functional dentition. If you qualify, procedures like scaling, surgery, implants (in some cases) may be covered. Veterans should check VA eligibility or dental insurance options.
Q: Is periodontal treatment painful for vets with anxiety/PTSD?
A: Modern periodontal care can be performed with effective anesthesia and sedation. Dentists often use local anesthetic injections and may offer nitrous oxide or oral sedatives. Because periodontitis affects overall health, treatment is worth it despite anxiety. Communicate fears with your dentist – many veterans benefit from calming techniques and an empathetic approach.
Q: Do smokers or diabetics get different periodontal care?
A: Smoking and uncontrolled diabetes both hinder healing. Smokers have higher failure rates of both therapy and implants, and diabetics have slower recovery. Treatment itself is similar, but extra measures are taken: patients are urged to quit smoking, and blood sugar should be controlled before surgery. In other words, vets with these conditions still get treated, but their conditions are managed in parallel to improve outcomes.
Call to Action: For veterans in Petersburg or Glen Allen needing gum disease care, contact United Smiles for personalized treatment plans. Schedule an appointment at our Petersburg office (34 Medical Park Blvd E, Petersburg, phone (804) 894‑9393) or Glen Allen office (5332 Wyndham Forest Dr, (804) 999‑9099). Our team will work with your VA benefits to provide effective therapy.
Comparison of Periodontal Treatments:
| Treatment | Description | Indications | Procedure Steps | Anesthesia | Recovery | Risks/Complications | Outcomes/Prognosis | Typical Cost | VA Coverage/Benefits | Suitability (Comorbidities) |
| Scaling & Root Planing (NSP Therapy) | Deep cleaning (SRP) of roots to remove plaque/tartar. May include local antibiotics. | Early/mild-to-moderate periodontitis (pockets ≤5 mm); first phase of therapy. | Quadrant-wise cleaning under local anesthetic. Ultrasonic/hand instruments “scale” deposits and “plane” roots. Oral hygiene instruction. | Local anesthetic (e.g. lidocaine). Sedation optional. | Minimal. Soreness 1–3 days. Cold sensitivity possible. | Gum recession (post-healing) and sensitivity; rare infection/abscess. Less effect if poor hygiene or smoker. | 1–3 mm pocket depth reduction in moderate cases. Moderate attachment gain. Most inflammation resolved; maintenance needed. | ~$200–$300 per quadrant (~$800–$1,200 full mouth). | Covered for eligible vets (Class I/II/IV: full care; Class IIA: as needed for function). | Well-tolerated by most. Advise smoking cessation, control diabetes. |
| Adjunctive Antimicrobials | Antibiotics or antiseptics added to NSPT (e.g. systemic doxycycline, local gels/chips). | Chronic periodontitis needing extra effect. | Systemic (oral antibiotics) or local (injected gels, medicated chips) added to SRP. | Same as SRP. | Same as SRP (plus drug side effects). | Antibiotic side effects (GI upset); potential resistance. | Small additional PD reduction/attachment gain over SRP alone. Not used routinely. | Varies (typically added to SRP cost). | Generally covered if part of prescribed treatment plan. | Caution if allergy; check med list (warfarin interactions). |
| Periodontal Maintenance (SPT) | Ongoing recall cleanings to prevent recurrence. | All periodontitis patients after active therapy. | Regular (3–6 months) visits with exam and cleaning. | None (sometimes topical anesthetic if scaling). | None/Minimal. Normal prophylaxis discomfort. | If skipped, disease often returns. | Sustains prior gains; reduces tooth loss long-term. | $100–$200 per visit. | Covered as preventive/follow-up care. | Critical for all; emphasizes self-care and quitting smoking. |
| Flap/Pocket Reduction Surgery | Surgical flap access to clean roots & reposition gum. Often with osseous resection. | Deep pockets (≥6 mm) or persistent infection after NSPT. | Incisions made; flap lifted; root surfaces debrided; possibly bone contoured; flap sutured. | Local anesthetic; optional sedation. | Moderate: 1–2 weeks. Swelling, pain managed with NSAIDs. Stitches at ~2 weeks. | Bleeding, infection, gingival recession, root sensitivity. | Significant pocket depth reduction (>3–4 mm in deep sites). Attachment level improves. Deeper teeth have better outcomes. | ~$800–$1,200 per quadrant. | Covered if needed to save teeth (Class I/II/IV, etc.). | Safe in older vets; heal slower if smoker/diabetic. Good hygiene crucial. |
| Osseous Resection Surgery | Reshapes/supporting bone for positive architecture. | Vertical bone defects <4 mm or flat bifurcations; crown lengthening. | After flap, bone peaks trimmed (ostectomy) and reshaped; bone files for smooth contour; flap sutured. | As above (flap). | Moderate: 1–2 weeks healing. Some extra discomfort from bone work. | Increased recession, dentin hypersensitivity, especially anterior region. | Pocket depth reduction of 3–5 mm in treated areas. Allows flat bone, stable healing. | Included with flap costs (~$800–$1,200 per quad). | Same as flap surgery (VA covers if indicated). | Avoid in aesthetic front teeth if possible. Additional recession expected. |
| Bone Grafting & GTR | Placement of bone graft material + barrier membrane to regrow bone. | Deep intrabony defects (≥4 mm), vertical bone loss, furcations (Class I-II). | Flap opened; clean defect; apply graft material (autograft/allograft/etc.) and membrane; flap sealed. | Local anesthetic. | Longer: Flap ~2 weeks; bone takes months. Strict care (no brushing for ~2 weeks on site). | Membrane exposure/infection; graft failure; swelling/pain. Smokers & diabetics hinder regeneration. | Potential bone fill of defect and 3–5 mm pocket reduction. Good if defect morphology favorable. | Grafts: ~$600–$1,500 per site; membranes add ~$300–$1,000. | Covered when needed to save tooth/bone. VA may review case for coverage. | Less predictable if patient smokes or has diabetes. |
| Crown Lengthening Surgery | Surgical exposure of more tooth for restorations by removing gum/bone. | Subgingival decay/fracture; inadequate tooth for crown; “gummy smile”. | Apical flap with ostectomy around tooth to expose 3–4 mm of root. | Local anesthetic. | 1–2 weeks for gums to heal. Temporary crown used for ~6 weeks post-surgery. | Longer-looking teeth; increased root exposure; may preclude implants on other teeth due to bone removal. | Successfully exposes needed tooth structure for restoration. Gingival margin stable after healing. | ~$500–$3,000 per tooth. | Covered as needed restorative prep. VA may require dentist justification. | Only if benefit outweighs aesthetic change. Avoid if it would expose a furcation or crucial bone. |
| Dental Implants | Surgical titanium posts & crowns to replace lost teeth. | Missing tooth/teeth due to periodontitis; patient desires fixed replacement. | (Often staged) Extract teeth, graft bone if needed, place implant (2–3 mo. healing), attach abutment and crown. | Local anesthetic; sedation often used. | Soft tissue ~1–2 weeks; osseointegration ~3–6 months. | Failure (implant doesn’t integrate), infection (peri-implantitis), nerve injury, sinus issues. | High success (90–95% at 5 yrs) in healthy patients. Functions like natural tooth. | ~$3,000–$5,500 per implant crown; grafting adds $400–$2,500. | Generally not covered except in specific service-related cases. | Poor fit for heavy smokers or uncontrolled diabetes. Hypertension, cardiac meds require caution (inform surgeon). |
Sources: Authoritative dental literature and guidelines including ADA and AAP position statements, Cochrane reviews and systematic analyses, VA policy documents, and dental health references. Local clinic info (United Smiles Petersburg/Glen Allen) has been used to ensure regional relevance.